Dr Matt's Newsletter November 9, 2022
Supporting healthy social interactions and diversity of health choices

This newsletter includes an introduction to a major problem with covid-19 vaccines: lack of efficacy and the major red flag of “negative efficacy” which has been found in many studies around the world. “Negative efficacy” means an INCREASED chance of testing positive after the vaccine. Fortunately, our body has an innate ability to heal itself, whether vaccinated or not :-).
Below are the items in today’s newsletter.
Humor of the week: Vaccine Effectiveness - going, going, gone…
Inspirational quote from Thich Nhat Hahn: cradling our suffering
Family Run Business - Whiffletree Farm: Pay them a visit for grass-fed animal products and egg laying hens - the gift that keeps on giving.
Music of the week – I want a New Drug!
Research of the week – Studies around the world have found that Covid vaccines increase people’s chances of testing positive on the “covid tests”. Fortunately other research has found that our immune system handles covid-19 quite well.
Yours truly, one moment at a time.
Matt Irwin
Humor of the week – Vaccine Effectiveness in 2021

Inspirational quote from Thich Nhat Hahn: resolving suffering
Thich Nhat Hahn gave many lessons about reducing suffering, and ironically one of the key elements is learning to live in harmony with our own. This is a lifelong practice and I have just as much continued work to do as anyone else. These two quotes summarize what our internal and external practice can help.
“If you know how to make good use of mud, you can grow beautiful lotus flowers. If you know how to make good use of suffering, you can grow happiness.”
“We have to learn how to embrace and cradle our own suffering and the suffering of the world, with a lot of tenderness.”
Here is a link to a talk he gave in 2013 about a dream he had where he was placed in a terrifically embarrassing and anxiety producing position. It shows how he generated a fun learning experience in his re-”treats”, a nd also how he taught that looking inside ourselves is the way to relieve suffering , rather than pointing out the “speck of dust in our neighbor’s eye”.
Family Run Business of the week - Give the gift that keeps giving – an egg laying hen
This week’s family run business is Whiffletree farm. My patients, Liz and Jesse Straight own and run Whiffletree Farm in Warrenton Virginia with assistance from their very cute and rapidly growing children. They raise healthy grassfed animals and you can purchase animal products, fresh eggs, and laying hens to have your own fresh eggs.
Below is a link to their page on buying egg laying hens, which are highly recommended by Dr Matt for your family’s health. Of course, you will also need a predator-safe chicken coop, and may need to check-in with neighbors first. If your local government does not allow home-based hens. maybe we can work to change their minds by giving them some free eggs 😊.
https://whiffletreefarmva.com/store/egg-laying-hens-for-sale
Music of the week – I want a New Drug! By Huey Lewis and the News - a parody of the “pill for every ill” mentality.
We often blame “Big Pharma” for the massive overemphasis on drugs and vaccines in our health system. However, people drive this with their powerful internal wish to use quick fixes to eliminate illness. Unfortunately the human body is infinitely complex, and not nearly as simple as the mechanistic-materialist worldview imagines. Huey Lewis and the News poked fun at this with a playful song back in 1984. Below are some lyrics – with medical lingo added in parenthesis:
I want a new drug
One that won't make me sick (no nausea or dyspepsia)
One that won't make me crash my car (no mental status changes or slowed reactions)
Or make me feel three feet thick (no lethargy or muscle weakness)
I want a new drug
One that won't hurt my head (no headache or withdrawal symptoms)
One that won't make my mouth too dry (no anticholinergic effects)
Or make my eyes too red (no histamine response)
One that won't make me nervous (no insomnia or irritability)
Wondering what to do
One that makes me feel like I feel when I'm with you.
Research of the week – Studies around the world have found that Covid vaccines increase people’s chances of testing positive on the “covid tests”. Other new research analyses continue to show that our immune system handles covid-19 quite well, especially when our healing system is supported instead of being undermined.
Many discussions of vaccine safety and efficacy use intense fear-based arguments. You have to decide which is more frightening, to get an illness with a risk of death or to get a vaccine with a risk of death, and intense pressure comes from both sides. When fueled by scary stories of bad outcomes, any issue can become frightening. However, basic medical ethics can help, and this demands that people have a right to decide for themselves what is the healthiest option.
It is fine for people to disagree about the best choice, but hopefully we can resolve to live with our differences and appreciate places where we do agree. For example, most people agree that healthy nutrition, exercise, mental health, and spiritual health all help our healing systems work better. No matter what political, ethnic, racial, or ideological group people are in they also agree that taking care of the sick and elderly is a basic part of humanity.
I wish I could guarantee that any choice is risk-free, but the only risk-free choice is to never get out of bed. Wait – hold it –staying in bed also has a lot of risks, not to mention that our quality of life would be reduced! Another thing to consider, as pointed out by the Near Death Experience research in my newsletter from All Soul’s Day on November 2nd, is that our long term risk of death is approximately 100%, and this knowledge can motivate us to live life as fully as possible.
The failure to reduce viral spread eliminates any potential ethical argument for mandating vaccination. But what about research showing increased covid-19 rates? Wouldn’t this give an ethical argument to prevent people from getting the vaccine? Although most people would refuse a vaccine if informed about this, I would still argue that people can make their own choice.
New study confirms extraordinarily low risk from covid-19:
Before discussing covid-19 vaccines, it is smart to start with the actual risk from the illness. A recent paper by experienced epidemiologists from Stanford University School of Medicine confirmed that people under 20 had an extremely low risk that may astound you, even lower than the risk from other common viral illnesses like RSV and influenza (Pezzulo et al 2022 - see references section at the end).
I wrote a series of research papers documenting this extremely low risk, and arguing that the risk would be even lower if people got “normal high-quality healthcare and caregiving” instead of social isolation, healthcare disruption, and solitary confinement. This experience happened to nearly all people around the world, but was especially harsh for people when they were diagnosed with covid-19. It only takes a few seconds of attention to this detail to realize that it would skew mortality and morbidity statistics quite a bit. People with fragile health suffer more from the isolation protocols than younger people, and this is a primary reason for the often cited “increased risk from covid-19 in the elderly”.
Imagine a 90 year old with poor hearing and vision, who cannot effectively use a cell phone, and who already has some heart and lung disease just by virtue of their advanced age. This is an image I have seen thousands of times in my 18 years as a hospice physician. Yet, amazingly, even the vast majority of these people survived after several weeks, months, and even over a year of social isolation. Usually they had to live through at least one period of solitary confinement for testing positive for covid-19, and many of our hospice patients tested positive multiple times.
The new study on the extraordinarily low risk of mortality was published online on October 13, 2022. It looked at comprehensive data from 38 countries around the world, and found the mortality for people under age 20 to be about 1 in 333,000. Yes, you read that correctly. No, I did not accidentally add three zeros at the end. The Stanford researchers included John Ioannidis, who has been following and publishing this data since early 2020 (Pezzulo et al 2022). This data came from earlier viral variants considered more dangerous than the current variants like Omicron, and was also before the vaccine was available. This means that any questionable protection from the vaccine is not a factor.
The risks for older people were higher, but still much lower than people imagine, and the risk from every illness is higher in he elderly. For the oldest group they studied, ages 60 to 69, they found a mortality risk of about 1 in 200. As stated above, this rate would be even less if the harm of covid-19 required quarantine and solitary confinement was accounted for, which is much more harmful to the elderly. Just as with other viral illnesses, underlying conditions such as metastatic cancer and advanced heart and lung disease are the primary culprits, no matter what virus people are diagnosed with.
The risk they found for young people, 1 in 333,000, is similar to US college students, later confirmed with youths under age 20, with a mortality less than 1 in 100,000 in both groups. I reviewed this data, which was also from early variants considered more dangerous than current variants, in prior papers (see refence section below), and that data was also pre-vaccine. The handful of college students who did die had other health issues that were more significant than their positive covid-19 test, and I was able to find quotes from primary sources describing the conditions they had. I also emphasized that hundreds of times more college students die each year from other preventable causes, many of which were made worse by the isolation and social disruption from the exaggerated pandemic response.
Many people have trouble wrapping their heads around this. Perhaps their beliefs have been locked in through a barrage of negative media images combined with crowd psychology which activated a group survival instinct. It is easy to point at others as being unreasonable, but we all share free floating anxiety, we all have deep fears of illness and death, and we all often lock our anxieties unfairly on things around us. I find that practicing "sitting with my anxiety" helps more than blaming things around me, and allows me to take more positive actions.
Below is a quote from the study abstract. I have included parentheses to illustrate the mortality risk more clearly, such as “1 in 333,000” for 0.0003%.
"We identified 40 eligible national seroprevalence studies covering 38 countries with pre-vaccination seroprevalence data. The median IFR (Infection Fatality Ratio) was 0.0003% at 0-19 years (about 1 in 333,000), 0.003% at 20-29 years (about 1 in 33,000), 0.011% at 30-39 years (about 1 in 9,000), 0.035% at 40-49 years (about 1 in 3,000), 0.129% at 50-59 years (about 1 in 775), and 0.501% at 60-69 years (about 1 in 200).
Multiple studies have found that vaccinated people have increased chance of testing positive on the “covid tests”. - A “Red Flag” that seemingly everyone prefers to ignore
I began writing up this data about 6 months ago. However, just as I thought the paper was nearing completion another study would appear, and then another and another. This happened five times, and each time I would spend about another 10 hours editing what I had written to include the new information. For this reason I mainly discuss two studies below, which I call “The Danish Study”, and “The New York Study”.
A major problem in summarizing the data is that the authors of the studies always tried to explain the results away by saying things such as "after getting the vaccine people went out more and were tested more often, so they were more likely to test positive". While this sounds reasonable, the opposite is more likely true, with unvaccinated people being tested much more often partly due to mandated regular screening tests. The authors also preferred to highlight the short term initial efficacy, as well as discussing “waning efficacy”, but ignored or quickly explained away the “negative efficacy” they found. In an Orwellian twist, the authors often used “waning efficacy” as a reason to call for more frequent booster doses.
However, even the initial efficacy is questionable because they usually do not count people as vaccinated until two weeks after the second dose. If the vaccine triggered people to test positive before then it would be counted as happening in "unvaccinated" people, causing a complete inversion of the actual finding. The same is true of any negative health outcomes caused by the vaccine, which would be expected to occur immediately after it is given, and be falsely credited to the “unvaccinated” group.
Regarding mandated screening tests in unvaccinated people, the CDC website had a very long list of people who should be screened a minimum of once per week. I just spoke today to a teacher in my practice who tested positive on a weekly screening test yesterday, on November 8th. She is not sick but the private school she teaches at still requires weekly tests because she is unvaccinated. I have had many college students in my practice who were forced to be tested weekly, and a college athlete who was forced to test three times per week. This three times per week testing was required for every single unvaccinated NCAA athlete in every US college, in every sport, for the entire 2021-2022 school year. The most frequent testing I saw was in a journalist and a professional NBA player in my practice who were both tested every single day. I just saw his 3 year old daughter this week, and she is very cute and healthy as well as being extremely tall for her age :-).
The Danish Study:
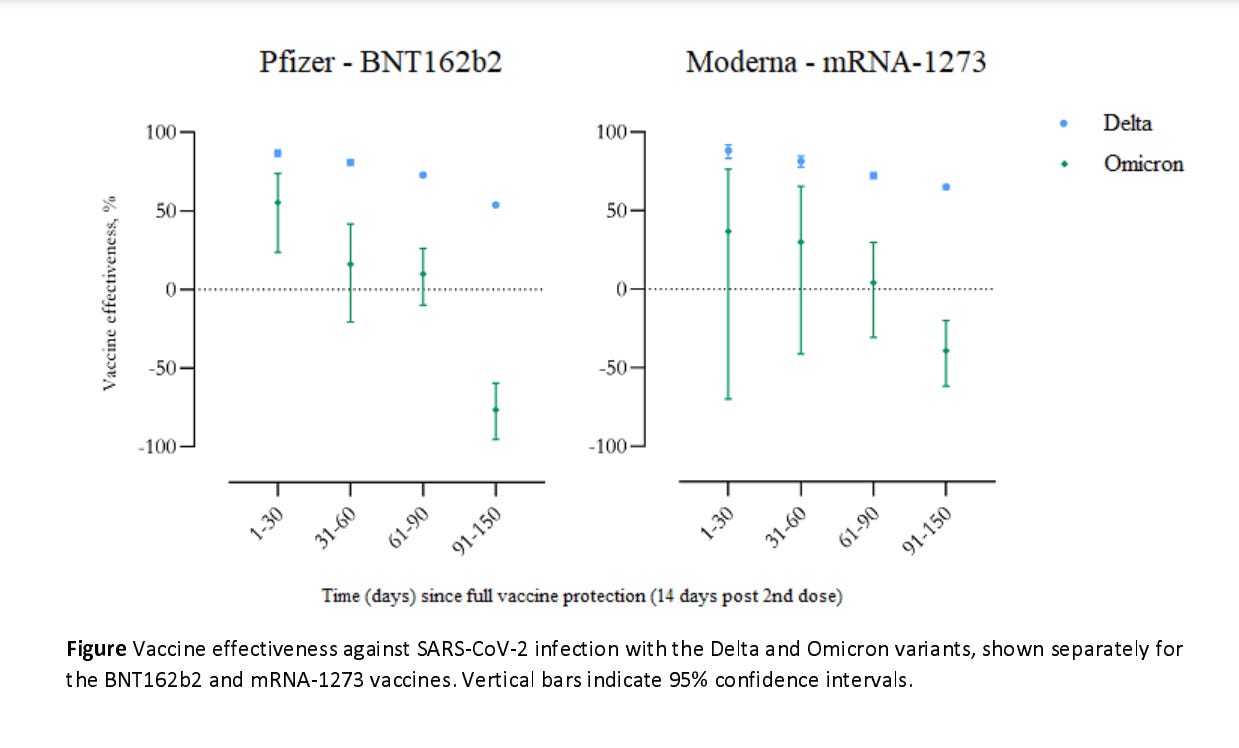
An example of a study finding increased positive rates is this large cohort study in Denmark which found an incredible 76.5% increase from the Pfizer vaccine, and 39.3% increase from Moderna, starting 3 months after vaccination. This was found during the Omicron wave and they claimed that it was more effective previous to this, but ignore the unequal testing rates discussed above.
Instead of conceding a major failure with their “negative efficacy” that appeared at the 90 day mark, the authors focus on the initial efficacy and call for more aggressive vaccination and more aggressive booster dosing, saying: “These findings highlight the need for massive rollout of vaccinations and booster vaccinations” (Hansen et al 2021 - link and graph below at the very end).
This study first came to my attention when an article by Nobel Prize Winner Luc Montagnier and a legal scholar wrote about it in a Wall Street Journal opinion piece in January 2022, calling the vaccine mandates unethical and illegal. They briefly mention specific research examples, saying:
“after 90 days, their effect went negative—i.e., vaccinated people were more susceptible to Omicron infection. Confirming this negative efficacy finding, data from Denmark and the Canadian province of Ontario indicate that vaccinated people have higher rates of Omicron infection than unvaccinated people,” (Montagnier and Rubenfeld 2022; emphasis in the original).
Several other studies have also shown a significantly increased risk of testing positive for covid-19, but often explain away the negative efficacy finding, focus on subgroups that had positive efficacy, or simply do not even mention the negative findings. These include a study of children in New York (Dorobawila et al. 2022), a study in Iceland (Eythorsson 2022), a study of Kaiser employees (Tseng et al 2021), and the study in the Canadian province of Ontario mentioned by Montagnier and Rubenfeld (Mason 2022).
New York Study of children (Dorobawila et al. 2022): The study from New York state found that kids age 5 to 11 had negative efficacy, with a 41% increased chance of testing positive on the covid-19 test when compared to unvaccinated kids. Older kids had “waning efficacy” that did not go below zero at 8 weeks when they stopped the study, but likely would have if they had continued. In all ages the efficacy was positive initially and waned quickly.
The authors emphasize the short term positive outcomes and a finding of reduced hospitalizations, and they do not even mention the increased risk of testing positive in their discussion or results sections. One has to look at Figure 2 (copied below at the very end) and understand that when the blue bar for ages 5–11 falls below 1, as it does at both 35-41 days and 42-48 days after they got the vaccine, it means they were more likely to test positive. Below the graph numerical results are shown, and one sees that at 35-41 days (5-6 weeks) efficacy was negative 10%, and at 42-48 days (6-7 weeks) it fell to negative 41% for ages 5-11. Both of these results were statistically significant. In the note below the figure they give the only mention of the negative results in an effort to discredit them, saying “Negative VE (Vaccine Effectiveness) values observed in later timepoints likely represent… residual confounding, as opposed to true relatively increased risk for those vaccinated”.
The New York study authors conclude that kids should get the vaccine because of an extremely small reduction in hospitalizations. However, unvaccinated children are more likely to be hospitalized than vaccinated children even with the exact same symptoms, and they are not even counted as vaccinated until two weeks after the second dose. This means that most hospitalizations caused by vaccine adverse effects would be counted as being in the “unvaccinated” group. The authors discuss the rapidly waning efficacy and use this to call for either more booster doses or a higher dosage of vaccine rather than recommending against it due to lack of efficacy and negative efficacy.
Increased positive testing immediately after the vaccine - i.e. the vaccine may trigger positive “covid tests”:
It is widely acknowledged that in the first week after being vaccinated people have a higher chance of testing positive, and this has also been found with booster doses. Although most people think this means an increased risk of infection, I am confident that they are false positives caused by a hyperactive immune system. This same phenomenon was recently found for the Monkeypox vaccine in a clinical trial in Chicago, with an incredible 1500 times increase in the chance of testing positive after people got the vaccine, which after adjusting for confounding variables dropped to only a 50-fold increased risk.
This incredible finding of 50-fold increased risk right after Monkeypox vaccination was discussed in an article by Madhava Setty (2022). Dr Setty spends most of his article in a detailed analysis of a large set of data from the United Kingdom showing “negative efficacy” of the covid-19 vaccine. The increased risk in the UK rose steadily from October 2021 to April 2022 until the increase reached 400 to 500% greater risk! In April the UK government abruptly stated they would not longer collect the data and stopped comparing vaccinated to unvaccinated populations, for obvious reasons.
Dr Setty is an anesthesiologist and was an electrical engineer for many years before a spiritual experience convinced him to go into health fields. On his website bio he states: “In the spring of 1992 I participated in a research expedition to the polar ice cap funded by the Office of Naval Research. That experience at the ‘top of the world’ completely changed my life. I was no longer willing to participate in any effort that wasn’t directed to the alleviation of suffering”. He has been a consistent critic of the covid-19 social isolation policies, with many papers, web-based presentations, and interviews. He also wrote a book about accessing intuition and the humility of learning, called “Woke”, which I have just ordered to my local Barnes and Noble. I prefer buying at local stores instead of online, and these days I always pay in cash :-).
Some mainstream articles have also discussed the issue of boosters causing increased covid-19 positive tests. For example, an article in the regular news media (CBS News - link below) stated: "For the week of April 23, it (the CDC) said the rate of Covid-19 infections among boosted Americans was 119 cases per 100,000 people. That was more than double the rate of infections in those who were vaccinated but unboosted, but a fraction of the levels among unvaccinated Americans... More boosted Americans may now have abandoned "prevention behaviors" like wearing masks, leading to an uptick... Some boosted Americans might be more likely to seek out a lab test for Covid-19, as opposed to relying on over-the-counter tests that go largely unreported to health authorities."
Although the writer of the NBC piece stated that the increased risk in boosted people was only "a fraction of the levels among unvaccinated Americans" this is patently false as shown by the studies discussed above. These studies found that people who are "unboosted but vaccinated" are usually much more likely to test positive than people who are completely unvaccinated, exactly the opposite of what the article claims. Any apparent initial reduction of risk in vaccinated people waned within weeks, and may have been due to counting newly vaccinated people as “unvaccinated” until two weeks past their second dose.
———————
Humility of learning helps all of us quite a bit, and I am still learning as I go just as they are, one step at a time.
References
Dorobawila et al. (February 28, 2022). Effectiveness of the BNT162b2 vaccine among children 5-11 and 12-17 years in New York after the Emergence of the Omicron Variant.
https://doi.org/10.1101/2022.02.25.22271454
https://www.medrxiv.org/content/10.1101/2022.02.25.22271454v1.full.pdf
Eythorsson et al (August 3, 2022). Rate of SARS-CoV-2 Reinfection During an Omicron Wave in Iceland. JAMA Netw Open. 2022;5(8):e2225320. doi:10.1001/jamanetworkopen.2022.25320 https://www.medrxiv.org/content/10.1101/2021.12.20.21267966v3.full.pdf
Hansen et al, (December 23, 2021). Vaccine effectiveness against SARS-CoV-2 infection with the Omicron or Delta variants following a two-dose or booster BNT162b2 or mRNA-1273 vaccination series: A Danish cohort study. https://www.medrxiv.org/content/10.1101/2021.12.20.21267966v3.full.pdf
Irwin M. (2020). Mortality rates in college students were found to be less than 1 in 100,000 back in autumn 2020, with older variants of covid-19 which are believed to be more dangerous than the newer omicron variant. This risk is very similar to what was found in Germany by Song et al.
Extremely low mortality in US college students and Swedish schools.
Irwin M. (2021). A large study in Germany by Song et al found mortality rates lower than 1 in 100,000 in children. In contrast, the risk of children dying from accidents and suicides is 100’s of times more likely in the US, and malnutrition causes 1000’s of times more deaths around the world in developing nations. https://www.drmattirwin.com/german.html
Katz E. (2022, August 17). The Biden Administration Ends COVID-19 Testing Aimed at Unvaccinated Workers: Employees will soon face the same safety protocols regardless of vaccination status. Government Executive.
Mason J. (April 23, 2022). The Evaporating Effectiveness of Covid-19 Vaccines Shown by the Newest Ontario Government Data
https://c2cjournal.ca/2022/04/the-evaporating-effectiveness-of-covid-19-vaccines-as-shown-by-the-newest-ontario-government-data/
Montagnier & Rubenfeld (January 22, 2022). Omicron Makes Biden’s Vaccine Mandates Obsolete: There is no evidence so far that vaccines are reducing infections from the fast-spreading variant. Wall Street Journal: Opinion. https://www.wsj.com/articles/omicron-makes-bidens-vaccine-mandates-obsolete-covid-healthcare-osha-evidence-supreme-court-11641760009
Pezzulo et al (2022). Age-stratified infection fatality rate of COVID-19 in the non-
elderly informed from pre-vaccination national seroprevalence studies
Setty M (2022). Why are we calling them breakthrough infections?
https://childrenshealthdefense.org/defender/breakthrough-infections-covid-vaccine-failure/
Tseng H et al (2021) Effectiveness of mRNA-1273 against infection and COVID-19 hospitalization with SARS-CoV-2 Omicron subvariants: BA.1, BA.2, BA.2.12.1, BA.4, and BA.5. (Study of Kaiser employees)
https://www.medrxiv.org/content/10.1101/2022.09.30.22280573v1
Why boosted Americans seem to be getting more COVID-19 infections
https://www.cbsnews.com/news/covid-19-vaccine-booster-shot-infection-rate/